The term, edema, denotes an increase in the extravascular component of the extracellular fluid volume. Before clinically recognizable edema becomes apparent, a considerable rise in the extravascular component occurs, resulting in an appreciable weight gain.
Two major forms of edema are generally recognized: localized and “generalized”. The gross generalized edema is often termed “anasarca”. Examples of localized edema include ascites, hydrothorax (which may be secondary to a systemic disease), excessive crying, conjunctivitis, insect bite, Milroy’s disease, etc. Examples of generalized edema include kwashiorkor, nephrotic syndrome, cirrhosis of liver, congestive cardiac failure (CCF), etc.
The patient’s history is important in the formulation of a differential diagnosis. In case of generalized edema of the newborn, specific questioning should include information on blood group incompatibility (hemolytic disease of the newborn). Any suggestion of congestive cardiac failure (as manifested by dyspnea, cyanosis, etc. besides edema), fulminant infection, cold injury, over- hydration/hypernatremia or maternal diabetes?
After the neonatal period, history should aim at specifically excluding malnutrition (both primary and secondary), renal disease, congestive cardiac failure and liver disease as the most allergy to aspirin or some other agent? Any history of subcutaneous potent causes of generalized edema. Also, is there any history of bleeding with abdominal pain or arthritis (anaphylactoid purpura)? Has there been excessive intake of sodium or fluid? Any predisposition to sodium retention (steroids)? Has the patient been recently started on treatment for diabetes mellitus?
In localized edema, specific questioning depends upon the site affected. For instance, edema of the face must elicit such information as excessive crying, excessive rubbing of the eyes, conjunctivitis, blephritis, allergy to eyedrops or some other agent, “congress” grass, i.e. perthinium), acute sinusitis, dental abscess, orbital cellulitis or cavernous sinus thrombosis. Is there any accompanying facial palsy with furrowed tongue (Melkersson’s syndrome)?
An edematous arm may be the result of arm presentation or its isolated exposure in cold environment.
Edema over feet and legs ever since birth is usually due to Milroy’s disease, or Turner’s syndrome.
GENERALIZED EDEMA
Generalized Edema in Newborn
Hemolytic Disease of Newborn
In the severest form of Rh hemolytic disease, hydrops fetalis, the baby is remarkably edematous with effusion in serous cavities and massive hepatosplenomegaly. He is usually born preterm and may die shortly after birth as a result of severe anemia and congestive cardiac failure. In case of death in utero, the baby is macerated. The placenta is invariably large and edematous.
Alpha-thalassemia may present as fatal hydrops fetalis or hemoglobin H disease in which only Bart hemoglobin and hemoglobin H are present.
Congestive Cardiac Failure (CCF)
Infrequently, generalized edema involving the feet, legs, sacrum and eyelids may be a sign of CCF in the newborn. The accompanying manifestations include tachypnea, irritability, feeding difficulty, poor weight gain, weak cry, tachycardia, hepatomegaly, cardiomegaly and gallop rhythm. A common finding is pneumonitis with or without collapse of a part of the lung. A clinical assessment of JVP is rather difficult because of the shortness of the neck and difficulty in securing a relaxed state in case of newborns.
Even in the absence of a murmur, the probability of newborn’s CCF being secondary to congenital heart disease should be seriously considered.
Cold Injury
Neonatal cold injury occurs most often in low birthweight infants as a result of exposure to freezing cold, or following a resuscitation procedure or a cold snap.
Clinical features include a low body temperature (30 to 35°C or even less), cold skin (color may, however, remain pink giving an erroneous impression of good health), lethargy, refusal to accept feed, oliguria and bradycardia. Over areas of edema, skin may become hard and fixed to the underlying structures. The so-called sclerema, may be confused with scleredema.
Complications of cold injury include hypoglycemia, acidosis and hemorrhagic manifestations, such as massive pulmonary hemorrhage.
Electrolyte Imbalance
Overhydration, excessive administration of sodium through oral or intravenous rehydration therapy or concentrated milk formula, and inadequate excretion of sodium by immature kidneys in preterm newborns may be accompanied by clinically detectable edema.
Hypokalemia also is likely to cause edema in association with other manifestations such as muscular weakness.
Excess solute load as a result of high protein formula may also be responsible for clinical edema, more so in a preterm infant.
Hypoallergenic formula in cystic fibrosis may result in edema in neonatal period.
Nutritional Edema
Anemia with hypoproteinemia, idiopathic hypoproteinemia and vitamin E deficiency may manifest with neonatal edema. Whereas idiopathic hypoproteinemia occurs in term infants, the remaining two conditions usually are encountered in preterm infants.
Renal Edema
In congenital nephrosis, the newborn may present with hypoproteinemia and edema. Two major types (1.Infantile microcytic disease-Finnish type, 2. Membranous nephropathy of congenital syphilis) are recognized.
Remaining causes include congenital toxoplasmosis, congenital rubella, nail-patella syndrome, etc.
Maternal Diabetes
The newborn of a diabetic mother is usually remarkably heavy, plump, full-faced, plethoric and covered with lot of vernix caseosa. He is prone to develop hypoglycemia, hypocalcemia, idiopathic respiratory distress syndrome (hyaline membrane disease), hyperbilirubinemia, renal and adrenal vein thrombosis and polycythemia. Incidence of congenital malformations is high.
Generalized Edema after Neonatal Period
Nutritional Disorders
Gross protein-energy malnutrition (PEM) in the form of kwashiorkor is by and large the most common nutritional disorder causing generalized edema in children, usually between the ages of 1 to 4 years (Fig. 20.1).
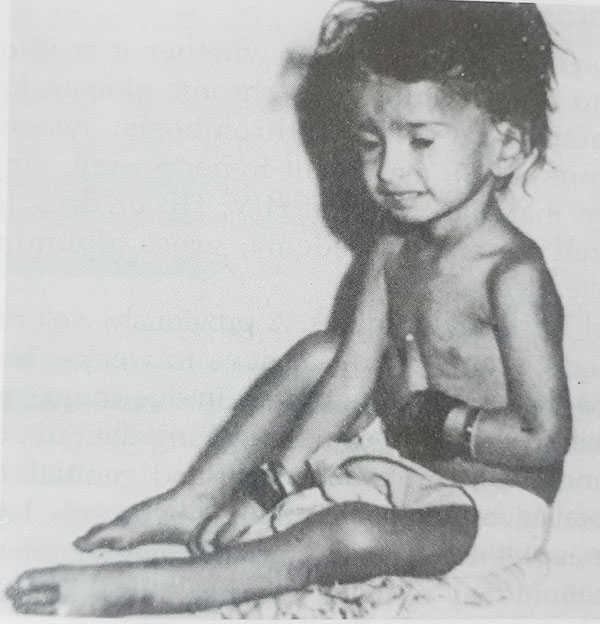
Fig. 20.1: Kwashiorkor Note the pedal edema, listlessness, muscle wasting with retention of some subcutaneous adiposity and growth retardation (weight 8.5 kg, height 72 cm) in this 2-year-old girl.
The fundamental nutritional inadequacy is primarily of proteins though energy deficiency and deficiencies of several vitamins and minerals also coexist. The essential features of the disease are growth retardation as evidenced by significantly low weight and height for age, gross muscle wasting with retention of some subcutaneous fat, mental apathy and edema (at least over pretibial region) with serum albumin less than 2.5 g%. The variable (nonessential) features include dermatosis, diarrhea, hepatomegaly, superimposed infections, hair changes and vitamin and mineral deficiencies. Marasmic-kwashiorkor refers to the state in which the child has gross wasting of muscles as well as subcutaneous fat (in short he looks marasmic), and also has developed edema.
Such conditions as celiac disease, cystic fibrosis, edemic tropical sprue, tuberculosis, hookworm disease and protein-losing enteropathy may cause secondary malnutrition and hypo-proteinemic edema.
Renal Disorders
Nephrotic syndrome, no matter whether it is idiopathic or secondary to such conditions as chronic glomerulonephritis, diabetes mellitus, renal vein thrombosis, systemic lupus erythematosus (SLE), malignant hypertension, amyloidosis, Plasmodium malarial infection HIV, HB or drug toxicity, is characterized by massive edema, gross albuminuria and hypercholesterolemia.
The onset is usually insidious. A previously well child begins to gain weight over a period of days to weeks. This may be accompanied by periorbital puffiness. In due course, he presents with massive generalized edema involving the face, extremities (Figs 20.2 and 20.3), trunk, abdomen, and genitalia, especially marked scrotal edema almost resembling hydrocele.
Hydrothorax and massive ascites may cause respiratory embarrassment. Edema of gut epithelium may result in diarrhea. Some hepatomegaly I usual. Blood pressure usually remains within normal range.
Acute nephritis is characterized by acute onset of fever, edema (most marked over face) and smoky or frankly bloody urine. Oliguria and hypertension are usually present. Occasionally, the
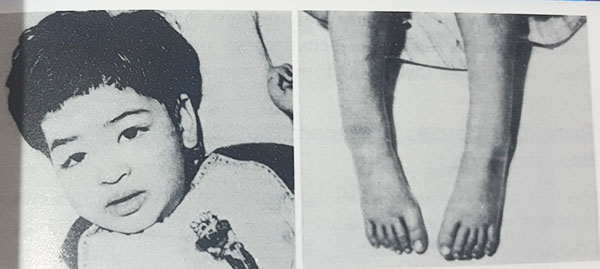
Figs 20.2 and 20.3: Nephrotic syndrome Note the periorbital puffiness and pedal edema. Urinalysis showed gross proteinuria Serum albuminuria was 2 g% and cholesterol 218 mg%.
child may present with hypertensive encephalopathy. Acute renal shutdown and CCF are other serious complications. Preceding these manifestations by I to 2 weeks is a streptococcal (beta-hemolyticus type 12) infection of throat or skin. Urinalysis reveals few to numerous red cells, many granular casts and mild to moderate albuminuria.
Remember that edema of acute nephritis is due to impaired function of the capillary wall. It, therefore, does not follow the hydrostatic pressure and does not accumulate in the dependent parts. Its characteristic sites are face, pretibial region and ankles.
Cardiovascular Disorders
Congestive cardiac failure may at times manifest with generalized edema. Remaining evidence of CCF in the form of dyspnea, basal crepitations and hepatomegaly should be looked for. Raised JVP is certainly an important finding but it may be quite difficult to detect it in infants.
You must ascertain the probable cause of CCF. The causes include congenital heart disease, rheumatic carditis, viral carditis, fibroelastosis and severe anemia.
Liver Disorders
Ascites, jaundice and hepatosplenomegaly characterize edema of Indian childhood cirrhosis, particularly in the second stage. Liver is typically firm with a sharp leafy margin. Superficial abdominal veins are quite prominent. Hematemesis or bleeding from other sites as a result of thrombocytopenia may occur. Anemia is quite pronounced.
Remaining Causes of Generalized Edema after Neonatal Period
Beginning of treatment of diabetes mellitus, overhydration and hypernatremia, aspirin sensitivity.
LOCALIZED EDEMA
Localized Edema in the Newborn
Head
Caput succedaneum is an edematous swelling, as a result of serosanginous collection from pressure over the presenting part between the pericranium and scalp tissue. It is present at birth, crosses the suture-line and disappears within a few hours to a day or so. It should not be confused with cephalhematoma in which swelling results from collection of blood between skull bone and overlying pericranium. It is, therefore, limited by suture lines. Regression takes a few weeks.
Face
Excessive crying, infections such as conjunctivitis or boils, and drugs (say sensitivity to eyedrops) may be responsible for edema of face and eyelids.
Limbs
Edema of an arm may well be due to arm presentation or exposure of the arm to low temperature. It may last several hours.
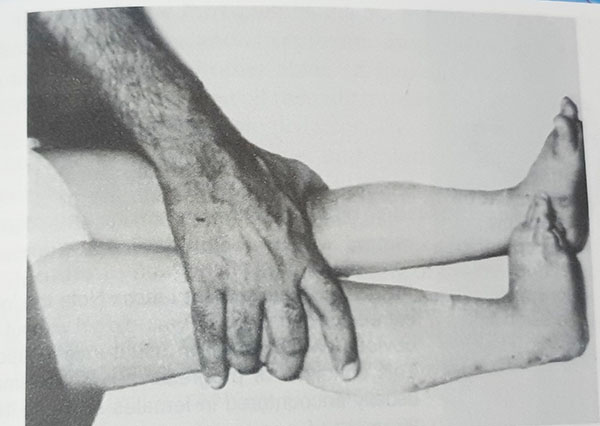
Non-pitting or pitting edema, often unilateral, present over legs ever since birth is in all probability Milroy’s disease (Fig. 20.4) It is predominantly lymphatic.
A characteristic edema of the dorsum of bands and feet in association with loose skin folds at the nape is a feature of gonadal dysgenesis, also termed Turner’s syndrome. Other manifestations of this 45, ‘X’ disorder at birth include a significantly low birthweight and low crown-heel length.
Fig. 20.4: Milroy’s disease The nonpitting edema in this child was present ever since birth.
Genitalia
Edema involving genitalia is a common finding in newborns. It is physiological and disappears without any intervention.
Some newborns develop a transient edema of scrotum. It may well be allergic in origin (say, sensitivity to detergents employed for washing the nappies), or due to insect bite or superficial cellulitis accompanying a pustule or abrasion. The edema and erythema tend to spread beyond the scrotum into the groin and perineum. As a rule, the manifestations are unilateral. This condition is accompanied by eosinophilia and usually responds to an antihistaminic agent like cetrizine. This poorly understood entity has been termed “idiopathic scrotal edema”.
Abdominal Wall
Edema of abdominal wall may accompany peritonitis, necrotizing enterocolitis and appendicitis in newborn. Edema in the last-named situation is localized to the right flank. At times, there is an associated erythema. Remaining manifestations include abdominal distention, irritability, vomiting and pyuria.
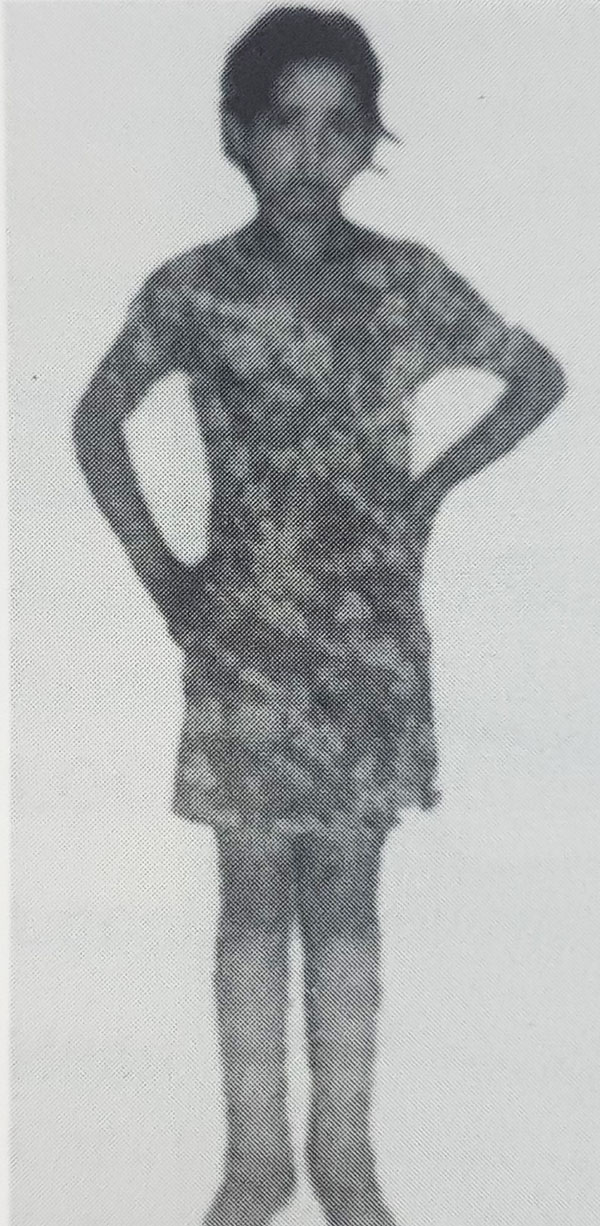
Fig. 20.5: Lymphedema precox Note the lower extremity edema in a 12-year-old girl without any obvious cause, even on usual investigations. This condition of progressive lymphedema is usually encountered in females between 10 to 25 years of age
Localized Edema after the Neonatal Period
Excessive crying, excessive rubbing of the eyes, conjunctivitis, blephritis and sensitivity to eyedrops or certain other drugs are common causes of edema about the eye.
Angioneurotic edema or Quincke edema results from an immune deficiency or secondary to a number of allergens including such agents as tatrazine (coloring matter in foods and drugs), disodium cromoglycate, demeclocycline and clonidine.
Face edema as a part of drug reaction may also occur in case of aspirin, cotrimoxazole, penicillin, nitrofurantoin, chlordi – zepoxide, cephaloridine, amitriptyline, clonazepam, etbosuximide, imipramine, primidone, troxidone and vitamin A toxicity.
Infections and inflammations such as boils, sinusitis, dental abscess, orbital cellulitis, chronic lymphangitis, resection of regional lymph nodes, filariasis, etc. are well known causes of localized edema (Fig. 20.5).
Mumps may be accompanied by edema over the manubrium (sternal edema) and upper chest wall as a result of lymphatic obstruction. It manifests some 5 days after the appearance of parotid swelling and lasts for almost an equal period.
Epidemic dropsy Infrequently, edema may result from adverse effect of a toxic substance. In epidemic dropsy which caused panic in Delhi and several other States of India in August-September 1998, consumption of an oil (usually mustard oil) adulterated with argemonex oil is the etiologic factor. The adulterant acts through a toxic alkaloid, sanguinarine, and interferes with oxidation of pyruvic acid that accumulates in blood. The seeds of the wild Argemone mexicana (the so-called “prickly poppy”) very much resemble the mustard seeds. The former has a tendency to grow in the thick of the latter. The intermixing of the two types of seeds, therefore, is understandable. In addition to its being accidental, it may also be done deliberately by unscrupulous elements.
Manifestations of epidemic dropsy include development of an acute non-inflammatory swelling in both legs, nausea and vomiting, diarrhea, dyspnea and congestive cardiac failure. A small number of subjects may develop flaucoma. Mortality in severe disease is high.
Diagnosis is primarily clinical and by exclusion of other causes of the clinical picture seen in dropsy. Two laboratory tests are available for establishing the diagnosis namely:
- Nitric acid test: It consists in adding nitric acid to a suspected sample. If argemone is present in at least 0.25% proportion, the sample will turn brown to orange-red.
- Paper chromatography It is the most sensitive and dependable parameter, gives positive result when mustard or some other oil contains as low when mustard or some other oil contains as low as 0.001% of argemone.
Treatment of dropsy is by and large symptomatic and supportive.