By definition, abdominal distention means enlargement or
protuberance of abdomen out of proportion to the body size as
a result of:
• Reduced tone of abdominal wall musculature
• Increased abdominal content, say fluid, gas or solid lump.
The term denotes a mere symptom that may not necessarily
mean a disease. As for instance, many small infants swallow fartoo-much of air when crying or during the course of a feed,
particularly when sucking is quite prolonged for one or the other reason. A protuberant abdomen is a common finding in normal,
healthy toddlers.
Ascites, i.e. fluid in the peritoneal cavity, tends to distend the
abdomen both in flanks and anteriorly, provided that it is
significantly large in quantity. In addition to fluid in the gut
(usually from obstruction or imbalance between absorption and
secretion), there is some accompanying gas as well (usually from
swallowed air or action of endogenous bacteria or other flora).
Audible gurgling noises may also be present.
Abdominal distention from gas in peritoneal cavity
(pneumoperitoneum) which may be accompanied by a tympanic
percussion note (yes, even on top of a solid organ like liver) points
to a perforation of a viscera. Mobile, nontender fecal lumps, i.e.
fecoliths, indicate severe constipation.
When confronting a child with abdominal distention, ask the
respondent about the general health of the child. Has he been doing
well, or not really been thriving satisfactorily? Is there history of
chronic/recurrent diarrhea and/or passage of worms in stools?
Does he has feeding problem? Any history of colic? Does he often.
Differential Diagnosis in Pediatrics
remain constipated? Any suggestion of swelling over face and legs?
Is the mother aware of any lump within the abdomen? Any
suggestion of emotional deprivation? Any drug intake?
Physical examination should aim at delineating if abdominal
distention appears to be the result of poor tone of the abdominal
wall musculature, or from gas, fluid or solid.
Abdominal Distention in the Newborn
The causes at this age include intestinal obstruction, rupture of
stomach or some other member of alimentary tract, biliary, or
urinary tract, tracheoesophageal fistula, congenital megacolon,
septicemia, peritonitis or necrotizing enterocolitis, congenital
nephrotic syndrome, tumors and cysts, congenital heart disease,
urethral obstruction, gray baby syndrome, etc.
Abdominal Distention in Infancy and
Childhood
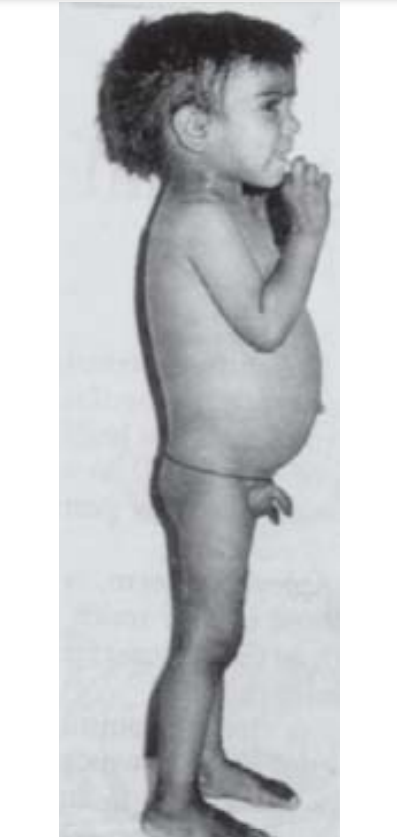
Fig. 1.1: Abdominal
distention in a 4-yearold with growth retardation and vitamin D
deficiency rickets.
The primary diagnosis in this child
was celiac disease.
Abdominal Distention
portal hypertension), pancreas (chronic pancreatitis), inferior vena
cava (thrombosis), lymphatics (tuberculosis, Hodgkin lymphoma)
as also in hypoproteinemic states like nephrotic syndrome, proteinlosing enteropathy, gross protein-energy malnutrition
(kwashiorkor type), cystic fibrosis and malabsorption states (celiac
disease).
Remember, ascitic fluid is generally a transudate with a low
protein concentration resulting from low plasma colloid pressure
(in hypoalbuminemia), from high portal-venous pressure or from
both. Usually, development of ascites accompanies significant fall
in serum albumin. Additional factors contributing to it include fluid
leak from lymphatics and visceral peritoneal capillaries. Furthermore, as the ascetic fluid collects, sodium excretion in urine greatly
falls. Thus, additional dietary sodium goes straight to the peritoneal
cavity.
Infrequently, when ascitic fluid is an exudate, i.e. with high
protein concentration, an inflammatory or malignant process must
be suspected.
Drugs such as diphenoxylate HCl, loperamide and
indomethacin are known to cause abdominal distention in some
subjects.
Remaining causes include paralytic ileus, intestinal obstruction,
perforation, mesenteric cyst, peritonitis, liver cysts and tumors,
hydronephrosis, polycystic kidney, renal vein thrombosis,
nephroblastoma (Wilms tumor), neuroblastoma, adrenal
hemorrhage, anterior meningocele, pancreatic cyst, leukemia,
tyrosinosis, Gaucher disease, porphyria, H. pylori infection, etc.
FURTHER READING
1. Wyllie. Major symptoms and signs of digestive tract disorders. In:
Kliegman RM, Behrman RE, Jenson HB, Stanton BF (Eds): Nelson
Textbook of Pediatrics, 18th edn. Philadelphia: Saunders 2008:1522-1528.
2. Green M. Pediatric Diagnosis, 6th edn. Philadelphia: Saunders 1998.