Constipation (Latin: constipare–to press together) refers to passage of small hard, dry stools that contain mainly solids and minimal water. Infrequency of defecation is usually associated. But that is not always so. The commonly-held belief that constipation means infrequency of defecation is, therefore, not correct
It is of value to understand that all pelvic and abdominal muscles play an important role in defecation. Nevertheless, three muscular sphincters surrounding the anus and the rectum (internal and external sphincters and puborectalis) are the most important (Fig. 11.1). When the conditions are condusive for defecation, the striated muscles of the pelvic flow and external sphincter are relaxed voluntarily, the anorectal angle is diminished and the abdominal muscles contract to facilitate the downward passage of stools. The main propulsive activity come through the nonperistaltic mass contraction of the colon
Two fundamental factors contributing to constipation are: (i) defects in emptying the rectum, (ii) defects in filing the rectum. Defects in emptying the rectum, leading to stool retention, may result from interference with defecation reflex initiated by pressure receptor in the rectal muscles. Lesions of the rectal muscles, sacral spinal cord afferent fibers, and the pelvic floor and abdominal muscles, and lesions that prevent adequate relaxation of anal sphincter fall in the group.
Defective rectal filing may be encountered whenever there is poor gut peristalsis (hypothyroidism, diphenoxylate, loperamide oropiate use), or there is mechanical structural lesion (Hirschsprung disease).
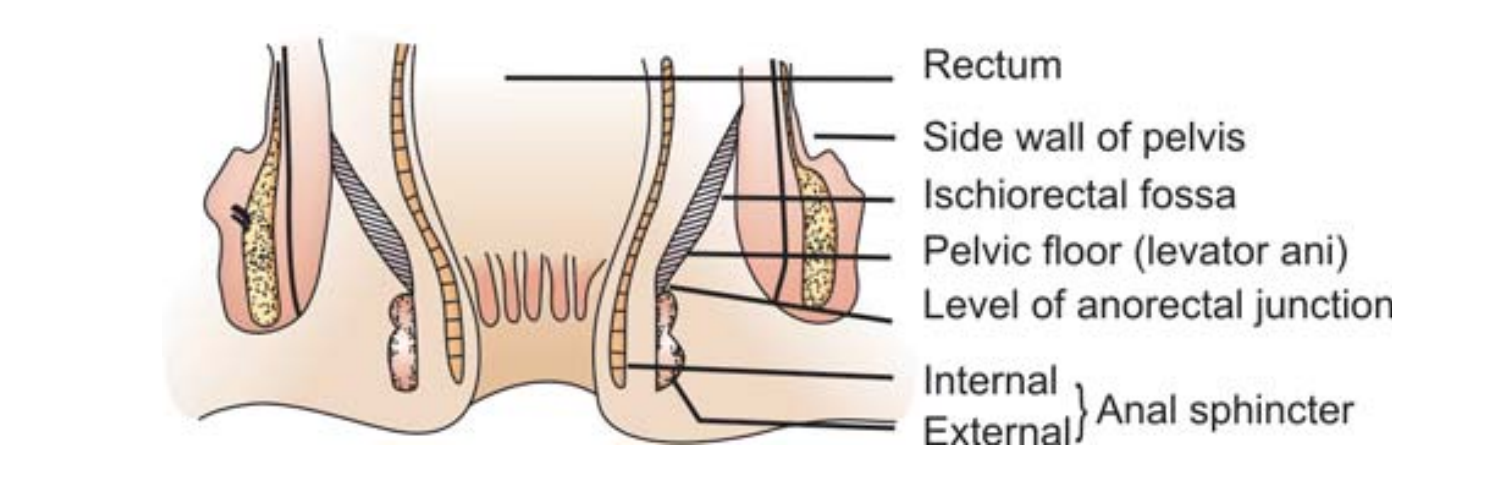
Fig. 11.1: Muscle involved in defecation (Reproduced from Sarin YK, Kaur G, Singh T: Constipation. In: Gupte S (Ed): Recent Advances in Pediatrics (Special Vol 6: Gastroenterology, Hepatology and Nutrition), New Delhi: Jaypee 2000: 213-226).
Both in defective emptying and filling, excessive drying of the stools follows. Hard, dry stools are rather painful to evacuate, leading to further retention. Thus a vicious cycle is set up. Constipation, therefore, tends to be self-perpetuating.
It is the anxiety on the part of the parents that may render constipation to have adverse effects (primarily on child’s emotional health) and not the constipation per se.
The following clarifications in the history are helpful in reaching the diagnosis: How long has the problem of constipation been? Is it ever since birth or occurred later? What is the child’s usual bowel habit and in which way has it changed? What is the frequency and consistency of motions? What are the feeding habits? Can the constipation be explained by the kind of diet? Any relationship with drugs, particularly laxatives or purgatives? Is there any associated pain with defecation or in the abdomen? What is the color of stools? Is there any vomiting? Any history of passage of worms in stools? Any fecal incontinence?
It is important to examine the abdomen for palpable numerous hard masses (fecolith). Anus and rectum in particular need to be inspected.
NEONATAL AND EARLY INFANCY
Benign
Breastfeeding
In the later neonatal period and early infancy, breastfed babies may pass stools only once in a few days. But, mind you, these stools are rather loose (like those the breastfed infant passes in early neonatal period) and seldom dry and solid. In true sense, this is not constipation. If a breastfed infant’s mother is consuming much-too-much of fats and proteins, his stools may be firmer and pultaceous.
Artificial Feeding
- Inadequate fluid intake, especially in hot weather
- Excessive sweating due to over clothing
- Inadequate sugar in the milk feed.
Delayed Weaning
Inadequate or delayed introduction of semisolid foods.
Medication
Abuse of laxatives/purgatives over a prolonged period by the parents obsessed by the desirability to have daily bowel movement, causing diarrhea alternating with constipation. Drugs like isoniazid, chlordiazepoxide, imipramine, amitryptaline and vincristine may cause constipation.
Organic
Obstructive/Mechanical Lesions
Imperforate anus is characterized by a cutaneous collection of meconium in the perineal region, presence of an anal fissure in place of opening and usually a fistulous opening in the perineum, into vulva or urethra. Anorectal stenosis occurs usually in association with other congenital anomalies and in preterm infants. There may be history of passage of stools resembling expelled toothpaste. A rectal examination needs to be done to confirm the diagnosis. Ectopic anus placed anteriorly may well be a common cause of constipation.
Meconium plug syndrome is characterized by passage of a sticky white plug of mucus followed by flatus and liquid meconium or delay in passage of meconium beyond 36 hours. Insertion of the little finger into the rectum release the meconium plug.
Meconium ileus, a common presentation in cystic fibrosis of pancreas, is characterized by feeding difficulty, abdominal distention, bilious vomiting between 34 to 48 hours of birth and fecal pellets (Fig. 11.2). Abdominal examination may reveal a palpable lump. X-ray abdomen (plain film) may show uneven dilated loops of bowel, air-fluid levels and a bubbly granular density. Barium enema may show micro colon from disuse.
Small left colon syndrome, resembling meconium plug syndrome, may occur mostly in infants of diabetic mothers and is due to disturbance of peristalsis.
Functional ileus of the newborn is characterized by manifestations of intestinal obstruction in the absence of any anatomical obstruction. It is secondary to septicemia, pneumonia, electrolyte imbalance and certain metabolic abnormalities. The condition is purely functional and occurs more often in the preterm infants. Hirschsprung disease usually manifests in the first week of life with failure to pass meconium, abdominal distention, bilious

Fig. 11.2: Fecal pellets in meconium ileus.
vomiting and feeding difficulty. Later, the pictures may be complicated by diarrhea secondary to enterocolitis. The infant fails to thrive satisfactorily. Rectal examination shows no fecal matter and the canal may feel narrow and tight. X-ray abdomen (plain film) shows gaseous distention whereas barium enema reveals a narrow distal segment and a dilated proximal segment of the colon and residual barium that may be detected 12 to 48 hours after the initial examination. The characteristic radiologic changes may manifest after 6 weeks of life. The diagnosis needs to be confirmed by rectal biopsy which demonstrates agangliosis, i.e. absence of ganglion cells of the submucous (Meissner’s) and intramural (Auerbach’s) plexuses.
Pseudo-Hirschsprung disease is a very rare cause of constipation in infancy. It usually manifests some years afterbirth. It results from poor tone of the colon, leading to dilatation but, unlike true Hirschsprung disease, here the rectum is full, bowel does not have a narrow segment and agangliosis is not seen. Encopresis (fecal soiling) is an important manifestation.
Severe vomiting, as encountered in congenital pyloric stenosis or possetting, may also cause constipation.
Polyurea as in diabetes insipidus (nephrogenic), renal acidosis or hypercalcemia usually due to hypervitaminosis D, renal tubular defects or hyperparathyroidism.
Hypokalemia may be responsible for constipation in infants who suffer from dysclectrolytemia following an attack of diarrhea.
Hypothyroidism should be suspected in an infant who is constipated and also has feeding difficulty, prolonged physiological jaundice, hypothermia, hypotonia, poor mother activity and umbilical hernia with or without facial features of the disease. Retarded bone age radiologically and T help to reach the diagnosis.
Severe hypotonia as in prune-belly syndrome characterized by congenital absence of the abdominal muscles.
Lead poisoning should be suspected in infants exposed to lead (say, lead paint flakes, artist’s paints, kajal or surma, fumes from batteries) and suffering from constipation in association with transient pain abdomen, resistant anemia, weight loss, irritability, vomiting, headache, personality changes and ataxia. A lead line over the gums is typical. Urine lead level of more than 85 mcg/ 24 hours is diagnostic.
LATER INFANCY AND CHILDHOOD
Benign
Poor Dietary Intake
Inadequate dietary roughage and large amounts of milk are by far the most common cause of constipation in later infancy and childhood. A therapeutic trial can demonstrate it.
Abuse of Laxatives and Purgatives
Parents, eager that the child must have a bowel movement daily, indulge in frequent administration of laxatives or purgatives to the child. As a result, he begins to be dependant on such a medication and unless it is given as a daily “ritual” he may pass constipated stools.
Poor Toilet Training
Parents, overanxious about the daily bowel movement, may force the child to sit on the “pottie” far too long against child’s wish. Others may examine each and every stool that the child passes quite critically, inducing the child to refuse to empty his bowels. Reactive constipation secondary to poor toilet training is most often seen in children whose mothers are overprotective, tense, anxious and indulgent and having tendency to use coercive methods. The fathers, on the other hand, are fond of exerting excessive discipline.
Organic
Intestinal Parasitosis
Though most parasitic infestations are known to cause diarrhea, at least L. giardia and hookworm may well cause constipation alternating with diarrhea. Since both the infestions are quite common in tropical settings, intestinal parasitosis should always be excluded in cases of constipation unless, of course, the cause is very obvious.
Anal Fissure
An anal fissure causes pain during defecation and thus, may lead to withholding of the stools. Later, even if the child tries he finds it difficult to empty such a heavily loaded rectum. There may follow dilatation of the colon proximal to it. Anal fissure may result from hard scybala per se.
Hirschsprung Disease
See Page 129.
Pseudo-Hirschsprung Disease
See Page 130.
Hypothyroidism
See page 130
FURTHER READING
- Dave S, Gupta DK. Hirschsprung’s disease and associated neuronal intestinal malformations. In: Gupte S (Ed): Recent Advances in Pediatrics-12. New Delhi: Jaypee 2002:47–65.
- Horvath K, King J. Major manifestations gastrointestinal disease. In: Gupte S, Horvalh K (Eds): Pediatric Gastroenterology, Hepatology and Nutrition. New Delhi: Peepee 2009.
- Thapa BR. Constiation and encopresis. In: Gupte S (Ed): Recent Advances in Pediatrics 2004:413-423.
4. Wyllie R. Major symptoms and signs of digestive tract disorders. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF (Eds): Nelson Textbook of Pediatrics,18th edn. Philadelphia: Saunders 2008: 1522-1528.