ABSTRACT
Dengue is the most important mosquito-transmitted viral disease in terms of morbidity and mortality. Dengue fever is caused by one of the four related, but distinct, Flavivirus serotypes (DEN 1–4), which are transmitted to humans by the Aedes aegypti mosquito. Infected humans are the main carriers and multipliers of the virus, serving as a source of the virus for uninfected mosquitoes. The disease is concentrated in urban and peri-urban environments in tropical and subtropical regions. Dengue cases can occur in any age group. Clinical symptoms range from mild fevers, to a severe and potentially life-threatening hemorrhagic disease. Prompt recognition of dengue is important for appropriate case management. Source reduction of the breeding habitats of the major mosquito vector, Aedes aegypti, is the best form of control. Quite a few types of dengue vaccines are in pipeline.
Key words:Aedes aegypti mosquito,Arthropod-borne flavivirus,Dengue fever,Dengue hemorrhagic fever,Dengue shock syndrome,Dengue vaccines.
INTRODUCTION
Dengue fever is an infectious tropical disease caused by the viruses belonging to the Flaviviridae family. It is an acute febrile illness characterized by biphasic fever, myalgia, arthralgia and rash.1 It is also called “breakbone fever”.
EPIDEMIOLOGY
Dengue has become a global problem since the Second World War and is endemic in more than 110 countries. Its incidence has increased dramatically since the 1960s. Currently WHO estimates, there may be 50 million cases of dengue infection worldwide every year.2 During epidemics, secondary attack rate may go up to 80–90%. A large proportion of dengue hemorrhagic fever, requiring admission, are children. Case fatality rate without proper treatment can exceed 20%.
The geographic spread of dengue is similar to that of malaria, but unlike malaria, dengue is often found in populated urban and residential areas of tropical nations. The spread of dengue is attributed to the expanding 2geographic distribution of dengue viruses and their mosquito vector. Improper household water storage and inadequate waste disposal are key risk factors in its spread.3
ETIOLOGY
Dengue viruses are an arthropod-borne flavivirus that comprises four distinct serotypes (DEN-1, DEN-2, DEN-3 and DEN-4), constituting an antigenic complex of the genus flavivirus, family Flaviviridae.4 As per National Vector- borne Disease Control Program, DEN 1 and DEN 2 serotypes are most widespread in India.
Dengue viruses are spherical lipid enveloped single stranded approximately 11kb RNA viruses measuring 50 nm in diameter. The envelope protein bears epitopes which are unique to each serotype.5
Dengue viruses are transmitted to humans through bites of infective female Aedes mosquitoes for whom the source is an infected person or monkeys as in some parts of the world (Fig. 1.1).
Aedes aegypti—also called the “tiger mosquito”—is a daybiter with limited flight range, and breeds in fresh water collected indoors and peri-domestically in tropical areas. The outbreaks coincide with the monsoon.6
The extrinsic incubation period for dengue virus in the mosquito can vary with temperature but typically is in the 1–2 week range. The intrinsic incubation period for dengue virus in the human host most commonly is 4 to 8 days.7
Infection with 1 DENV produces lifelong immunity against reinfection with that DENV type but no long-term cross-protection against the other 3 DENV types (any cross-protection is ≤2 months).8
PATHOPHYSIOLOGY
The key features that determine the disease severity are plasma leakage and abnormal hemostasis leading to rising hematocrit, thrombocytopenia and varying degrees of bleeding manifestations.9 The cause of abnormal plasma leakage is still unclear but appears to be the result of cytokine production.
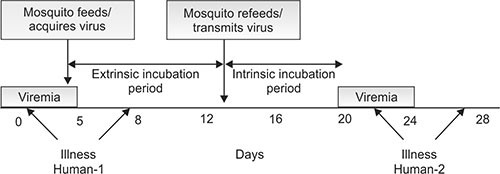
Fig. 1.1: Transmission and progress of dengue infection 3
The cross-reaction of antibodies generated against dengue virus proteins (especially NS1) results in thrombocytopenia. There is also activation of blood clotting and fibrogen pathways leading to disseminated intravascular hemolysis.10
SYMPTOMS
Typically, people infected with dengue virus are asymptomatic (80%) or only have mild symptoms such as an uncomplicated fever. Others have more severe illness (5%), and in a small proportion it is life-threatening (Fig. 1.2).1
The incubation period (time between exposure and onset of symptoms) ranges from 3 to 14 days, but most often it is 4 to 7 days. There may be abrupt onset of high-grade fever, facial flushing, headache, anorexia, vomiting and right hypochondriac pain. All patients have varying degrees of hemorrhagic manifestations like positive tourniquet test, petechial spots, epistaxis, GI bleed and rarely hematuria or intracranial bleeds.11
There are 3 phases of disease due to dengue virus infection, the febrile phase, critical phase, and recovery phase.12–13
The febrile phase is characterized by high fever, headache, generalized arthralgia and myalgia; thus the “breakbone” description. Progressive leukopenia is noted and petechiae and bleeding from mucous membranes may occur.
In the critical phase we see defervescence, progression of leukopenia, and thrombocytopenia. Importantly, we see an increase of capillary permeability leading to a plasma leakage—this is primary indicator of the severity of disease. Abdominal pain is often a sign of plasma leakage, if uncorrected by intravenous rehydration, plasma leakage can lead to metabolic acidosis and disseminated intravascular coagulation, resulting in a high risk of death.
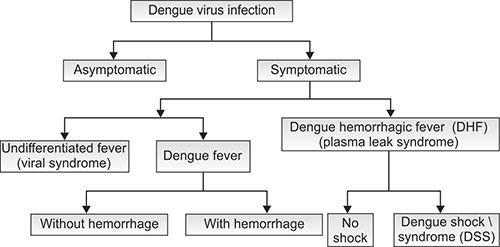
Fig. 1.2: Clinical presentations of dengue fever (Source: WHO 1997 Dengue hemorrhagic fever: Diagnosis, Treatment, Prevention and Control, 2nd edition)
During the recovery phase, we see a resorption of leaked plasma. The hemodynamic status stabilizes, and the urinary output increases. There is an overall clinical improvement. It is very important to note that the prevention of fluid overload during the recovery phase is critical, as this is a preventable cause of death in severe dengue.
Progression of clinical and laboratory features of dengue fever is depicted in Figure 1.3.
Dengue can occasionally affect several other body systems, either in isolation or along with the classic dengue symptoms. A decreased level of consciousness may occur in severe cases, which is attributable either to infection of the brain by the virus or indirectly as a result of impairment of vital organs, for example, the liver (Fig. 1.5).14
Dengue Hemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS)
These are severe forms of the dengue virus infections. These can occur in any age group even in infants.
Risk factors include15
- Virus type: DENV-2>DENV-3>DENV-4>DENV-1
- Preexisting antidengue antibody
- Age of host: Younger children at greater risk
- Secondary infection
- Genetics: Some people are resistant, may be due to some dengue resistant gene
- Hyperendemicity: 2 or more strains may be circulating simultaneously.
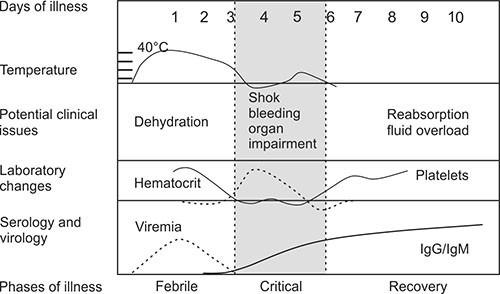
Fig. 1.3: Progression of clinical and laboratory features of dengue fever
In the 1997, WHO classification divided dengue into undifferentiated fever, dengue fever, and dengue hemorrhagic fever. Dengue hemorrhagic fever was subdivided further into grades I–IV (Fig. 1.4).16
Grade I is the presence only of easy bruising or a positive tourniquet test in someone with fever
Grade II is the presence of spontaneous bleeding into the skin and elsewhere
Grade III is the clinical evidence of shock, and
Grade IV is shock so severe that blood pressure and pulse cannot be detected.
Role of Tourniquet Test
This test is performed by inflating an appropriate size blood pressure cuff to a midpoint between the systolic and diastolic pressure for five minutes. A positive reading is taken as > 20 petechiae per 2.5 cm2 area. The test may be negative or only mildly positive in dengue shock syndrome.16
NEW (2009) DENGUE CASE CLASSIFICATION17
The World Health Organization’s 2009 classification divides dengue fever into two groups: uncomplicated and severe. This replaces the 1997 WHO classification, which needed to be simplified as it had been found to be too restrictive. However, the older classification continues to be used by many professionals.
LABORATORY INVESTIGATIONS
Thrombocytopenia (<100,000 cells/mm3) and hemo-concentration (hematocrit > 20% above the standard for age, sex and population baseline or baseline hematocrit) are common.
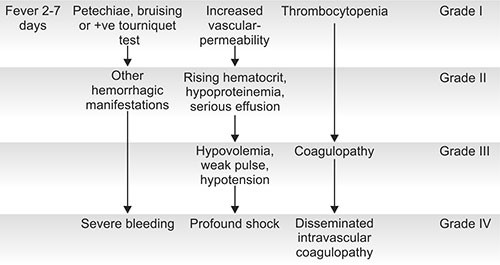
Fig. 1.4: Grading of dengue hemorrhagic fever
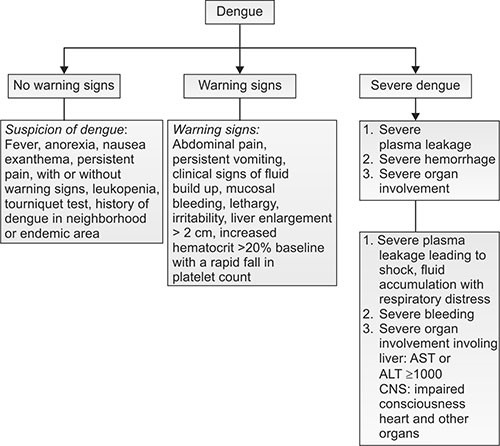
Fig. 1.5: Signs arousing “suspicion”, “warning signs” and signs suggesting “severe dengue”
Chest X-ray may reveal pleural effusion.
There may be hypoalbuminemia and raised transaminase levels on biochemical investigations.18
The diagnosis of dengue fever may be confirmed by microbiological laboratory testing. This can be done by virus isolation in cell cultures, nucleic acid detection by PCR, viral antigen detection (such as for NS1) or specific antibodies (serology). Virus isolation and nucleic acid detection are more accurate than antigen detection, but these tests are not widely available due to their greater cost. Detection of NS1 during the febrile phase of a primary infection may be greater than 90% however is only 60–80% in subsequent infections. All tests may be negative in the early stages of the disease. PCR and viral antigen detection are more accurate in the first seven days.17,19
Tests for dengue virus-specific antibodies, types IgG and IgM, can be useful in confirming a diagnosis in the later stages of the infection. Both IgG and IgM are produced after 5–7 days (Fig. 1.6). The highest levels (titers) of IgM are detected following a primary infection, but IgM is also produced in reinfection. IgM becomes undetectable 30–90 days after a primary infection, but earlier following re-infections. IgG, by contrast, remains detectable for over the 60 years and, in the absence of symptoms, is a useful indicator of past infection.
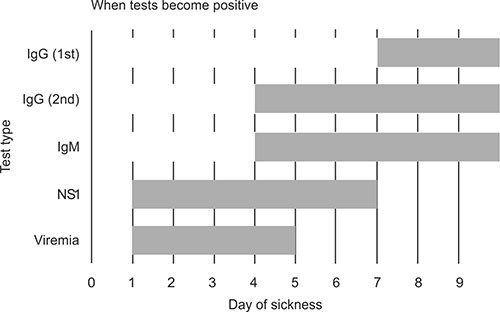
Fig. 1.6: Positivity of tests for dengue virus-specific antibodies
After a primary infection IgG reaches peak levels in the blood after 14–21 days. In subsequent re-infections, levels peak earlier and the titers are usually higher.12,19
Both IgG and IgM provide protective immunity to the infecting serotype of the virus. The laboratory test for IgG and IgM antibodies can cross-react with other flaviviruses and may result in a false positive after recent infections or vaccinations with yellow fever virus or Japanese encephalitis.13
TREATMENT17,18
Management of dengue fever is symptomatic and supportive. Bed rest is advisable during acute phase. Use tepid water sponging or antipyretic like paracetamol to control fever. There are no specific antiviral drugs for dengue, however maintaining proper fluid balance is important. Treatment depends on the symptoms, varying from oral rehydration therapy at home with close follow-up, to hospital admission with administration of intravenous fluids and/or blood transfusion. Intravenous hydration is usually only needed for one or two days. The rate of fluid administration is titrated to a urinary output of 0.5–1 mL/kg/hr, stable vital signs and normalization of hematocrit.20
Volume replacement flow charts for DHF with > 20% increase in HCt and DSS are given in Figures 1.7 and 1.8, respectively.
Blood transfusion is initiated early in patients presenting with unstable vital signs in the face of a decreasing hematocrit, rather than waiting for the hemoglobin concentration to decrease to some predetermined “transfusion trigger” level.
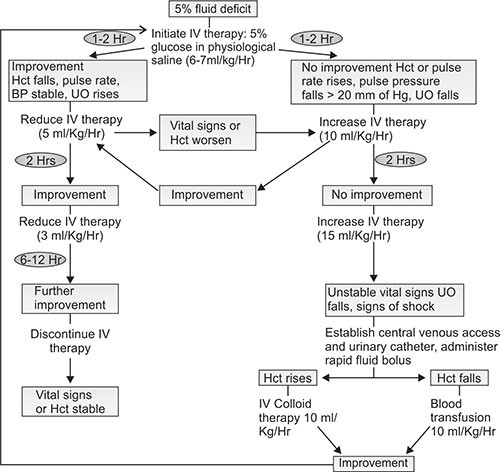
Fig. 1.7: Volume replacement flow chart for a patient with DHF and > 20% increase in HCt
Patients with dengue hemorrhagic fever or dengue shock syndrome may be discharged from the hospital when they meet the following criteria:
- Afebrile for 24 hours without antipyretics
- Good appetite, clinically improved condition
- Adequate urine output
- Stable hematocrit level
- At least 48 hours since recovery from shock
- No respiratory distress
- Platelet count greater than 50,000 cells/μL and stable hematocrit without intravenous fluids.23
MONITORING
Close monitoring of the patient is quite critical especially in first few hours. Vitals need to be measured every 30 minutes till they stabilize and thereafter every 2 hrs. Central venous monitoring should be done in children with features of shock.
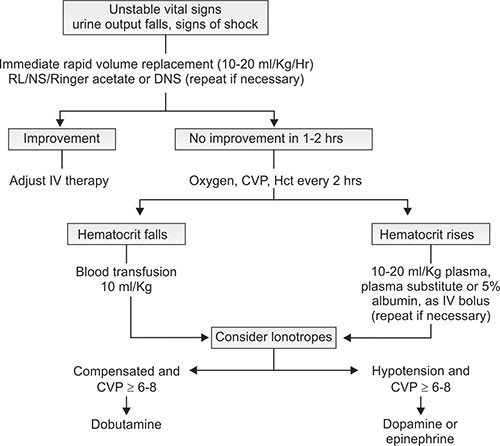
Fig. 1.8: Volume replacement flow chart for a patient with DSS
Hematocrit needs to be measured every 2 hr for 1st 6 hrs or until stable. Platelets are done daily till they show a rising trend.
PROGNOSIS
If left untreated, the mortality in patients with DHF or DSS may be as high as 40 to 50%. Early recognition, careful monitoring and appropriate fluid therapy has resulted in mortality rate to 1 to 5%.20 Prognosis is poor in patients with prolonged shock. So, early recognition of shock is of paramount importance.
PREVENTION20–23
Prevention depends on control of and protection from the bites of the mosquito that transmits it. Reducing open collections of water through environmental modification is the preferred method of control, given the concerns of negative health effect from insecticides and greater logistical difficulties with control agents. People can prevent mosquito bites by wearing clothing that fully covers the skin, using mosquito netting while resting, and/or the application of insect repellent (DEET being the most effective).10
As of 2013, there are no approved vaccines for the dengue virus. A number of vaccines are undergoing testing. The most promising one is based on a weakened combination of the yellow fever virus and each of the four dengue serotypes. It is hoped that the first products will be commercially available by 2015.
KEY LEARNING POINTS |
|
· Dengue is a mosquito-borne viral infection. Dengue results from infection with one of four distinct serotypes: DENV-1, DENV-2, DENV-3, and DENV-4. |
|
· The global incidence of dengue has grown dramatically in recent decades. About half of the world’s population is now at risk. |
|
· The most common outcome after infection by the bite of an Aedes mosquito (which bites in the day time) is asymptomatic infection, a flulike illness, or classic self-limited dengue fever. Severe, life-threatening disease with hemorrhagic manifestations or shock is rare. |
|
· Obtaining a history of the recent travel to a dengue-endemic area is a key in evaluating a person presenting with undifferentiated fever or a fever-rash-arthralgia syndrome. |
|
· Diagnostic testing is based on the natural history of infection; antibody levels begin to rise as levels of viremia begin to decline. |
|
· Risk factors help predict who will develop severe dengue after primary or secondary infection. |
|
· There is no specific treatment for dengue/severe dengue, but early detection and access to proper medical care lowers fatality rates below 1%. |
|
· Dengue prevention and control solely depends on effective vector control measures. |
REFERENCES
- Whitehorn J, Farrar J. Dengue. Br Med Bull 2010;95:161–173.
- Gubler DJ. Epidemic dengue/dengue haemorrhagic fever as a public health, social and economic problem in the 21st century. Trends Microbiol 2002;10:100–103.
- Gubler DJ. Dengue viruses. In: Mahy BWJ, Van Regenmortel MHV (eds): Desk Encyclopedia of Human and Medical Virology. Academic Press Boston: 2010: 372–382.
- Holmes EC, Twiddy SS. The origin, emergence and evolutionary genetics of dengue virus. Infect Genet Evol. 2003;3:19–28.
- Guzman MG, Kouri G. Dengue: Diagnosis, advances and challenges. Int J Infect Dis. 2004;8:69–80.
- Chopra A, Gandhi AK. Dengue-like illnesses in India. In: Gupte S (ed): Recent Advances in Pediatrics-15. Jaypee New Delhi: 2005:214–228.
- Gubler, Duane J. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev 1998;11:480–496.
- Gupte S, Shaik FA, Green J, Singh UK. Dengue. In: Gupte S, Gupte N (eds): Pediatric Infectious Diseases. Macmillan Gurgaon: 2012:181–202.
- Nimmannitya S. Dengue hemorrhagic fever: Disorders of hemostasis. Proceedings, IX Congress of the International Society of Hematology Asia-Pacific Division, 1999: Bangkok184–187.
- Falconar AK. Monoclonal antibodies that bind to common epitopes on the dengue virus type 2 nonstructural-1 and envelope glycoproteins display weak neutralizing activity and differentiated responses to virulent strains: implications for pathogenesis and vaccines. Clin Vaccine Immunol 2008;10:549–561.
- Farrar J. Clinical features of dengue. In: Halstead SB (ed): Dengue. Imperial College Press London: 2008:171–191.
- Chen LH, Wilson ME. Dengue and chikungunya infections in travelers. Curr Opin Infect Dis 2010;23:438–444.
- Simmons CP, Farrar JJ, Nguyen V, Wills B. Dengue. N Engl J Med 2012;366:1423–1432.
- Gould EA, Solomon T (February 2008). Pathogenic flaviviruses. Lancet 2008;371 (9611): 500–509.
- Vaughn DW, Barrett A, Solomon T. Flaviviruses (yellow fever, dengue, dengue hemorrhagic fever, Japanese encephalitis, West Nile encephalitis, St. Louis encephalitis, tick-borne encephalitis). In: Mandell GL, Bennett JE, Dolin R (eds): Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 7th edn. Elsevier/ Churchill-Livingstone Philadelphia: 2009:153–173.
- World Health Organization. Dengue Hemorrhagic Fever: Diagnosis, Treatment, Prevention and Control, 2nd edn. WHO Geneva: 1997:12–23.
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control. WHO Geneva: 2009: 10–11.
- Ranjit S, Kissoon N. Dengue hemorrhagic fever and shock syndromes. Pediatr Crit Care Med 2011;12:90–100.
- Guzman MG, Halstead SB, Artsob H. Dengue: A continuing global threat. Nat Rev Microbiol 2010;8(12 Suppl):S7–S16.
- World Health Organization. Global Strategy for Dengue Prevention and Control. WHO Geneva: 2012.
- World Health Organization. Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Hemorrhagic Fever. WHO Regional Office for South-East Asia New Delhi: 2011.
- Guy B, Barrere B, Malinowski C, Saville M, Teyssou R, Lang J. From research to phase III: Preclinical, industrial and clinical development of the Sanofi Pasteur tetravalent dengue vaccine. Vaccine 2011;29:7229–7241.
- Adhisivam B, Vishnu Bhat B. Vector-borne diseases. In: Gupte S, Gupte SB, Gupte M (eds): Recent Advances in Pediatrics (Special Vol 22: Immunology, Infections and Immunization). Jaypee New Delhi: 2013: 313–339.